
Pulsatile tinnitus (hearing your heartbeat) that began after a car accident, fall, or sports impact can be driven by more than “stress” or the ear alone. When symptoms change with head position, posture, or neck fatigue, the driver may be motion-dependent upper cervical mechanics. Digital Motion X-Ray (DMX) is motion-based fluoroscopic video imaging that evaluates real-time cervical segment behavior (translation and angulation) during guided movement, helping providers decide whether instability or hinge patterns may be contributing especially when MRI/CT are unrevealing.
- Pulsatile tinnitus that changes with head position, pressure, or posture can be motion-dependent.
- Standard imaging (MRI/CT/static X-rays) is valuable but often static; DMX evaluates function in motion.
- Motion findings can guide stabilization-first rehab, safer manual technique selection, and coordinated referral decisions.
Last updated: April 14, 2026
Reviewed by: DMX Miami clinical team
Pulsatile tinnitus is different from ordinary ringing. Patients describe it as “a whoosh,” “a thump,” or “I can hear my heartbeat in my ear.” In South Florida Miami, Fort Lauderdale, Miami-Dade County, Broward County, and the Florida Keys we see people develop pulsatile tinnitus after rear-end collisions, falls, or sports impacts. We also see out-of-town patients who travel through Florida from the USA and from Colombia, Chile, Argentina, Mexico, and the Caribbean looking for answers when the workup feels incomplete.
Important: pulsatile tinnitus can have vascular and neurological causes that require medical evaluation. This article is educational and is not a diagnosis. If you have sudden onset pulsatile tinnitus, neurological symptoms, vision changes, fainting, severe headache, or new weakness, seek urgent medical care.
Why pulsatile tinnitus can be “neck-driven” in some cases
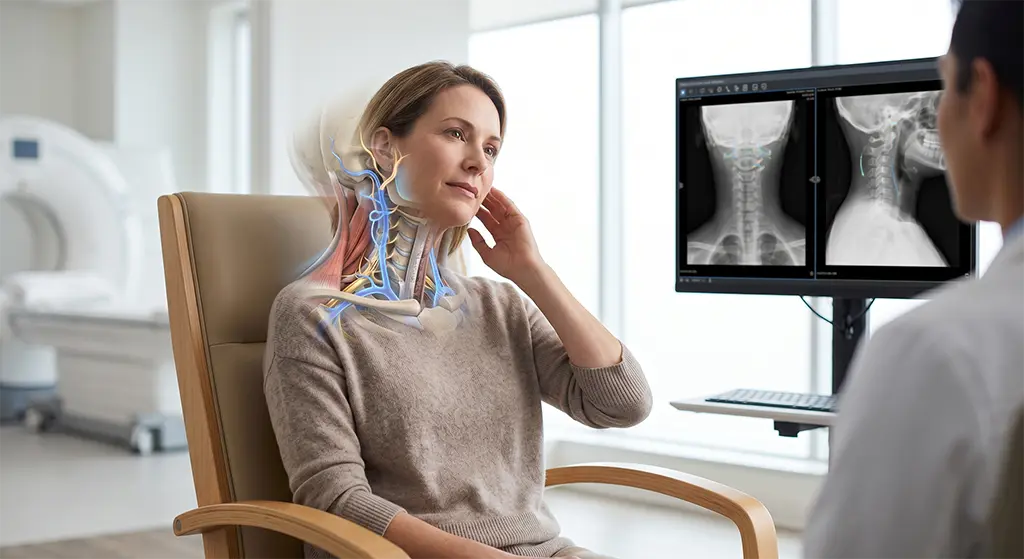
Your ears sit near a dense neighborhood of structures: the upper cervical spine, cranial nerves, arterial and venous pathways, and muscles that influence head posture. After trauma, the body often adopts protective patterns guarding, altered head position, and movement avoidance. If the upper cervical spine becomes motion-sensitive, the nervous system can respond with symptoms that feel “ear” related, especially when symptoms change with position.
A key clue: the symptom is position dependent
Many patients with a mechanical component notice at least one of these:
- symptoms change when they look up, look down, or rotate.
- symptoms change when they press on the side/front of the neck.
- symptoms change with posture load (driving, laptop work).
- symptoms worsen as the day goes on (neck fatigue / “heavy head”).
- symptoms improve temporarily with traction, specific positions, or manual work, then return.
Position dependence doesn’t prove the neck is the cause but it strongly suggests motion and mechanics should be evaluated as part of the larger picture.
Why static imaging can be normal when symptoms are real
MRI and CT are essential tools. They can identify many serious causes of pulsatile tinnitus, including vascular anomalies, mass lesions, and other structural issues. However, most MRI/CT studies are taken in still positions. If the symptom is driven by how segments behave during motion translation (sliding) and angulation (tilting) a static study may not capture the trigger.
Static imaging may miss:
- subtle instability that appears only during movement arcs.
- left-right asymmetry that emerges during rotation.
- hinge behavior (one segment moving too much while others remain stiff).
- sequencing issues (a segment “jumps” early in the arc).
What Digital Motion X-Ray (DMX) evaluates
DMX is fluoroscopic video X-ray performed with guided motion. It is not a replacement for MRI/CT. It answers a different question: what happens during the movement arc?
In cervical studies, providers often evaluate:
- Translation: how much one vertebra shifts relative to another during motion.
- Angulation: how much one vertebra tilts relative to another during motion.
- Symmetry: left vs right movement behavior.
- Hinge patterns: where motion concentrates and whether it matches the patient’s trigger.
- Global sharing: whether the neck distributes motion smoothly.
Why the upper cervical spine is often relevant
The upper cervical region (C0–C1–C2) is designed for mobility and fine control. After trauma, protective bracing can change how that region shares motion with the rest of the neck. If one level becomes a hinge point or exhibits abnormal translation/angulation, symptoms can become highly motion dependent.
Some patients also report associated symptoms such as:
- headaches at the base of the skull.
- visual strain or “pressure” with posture load.
- dizziness in busy environments.
- neck tightness that builds through the day.
These patterns don’t confirm a diagnosis, but they support the idea that a motion-based assessment may be useful.
How DMX findings can change the care plan
DMX is most valuable when it changes decisions. Depending on findings, providers may shift toward:
1) Stabilization-first rehabilitation
If motion suggests instability or hinge dominance, the priority is often controlled stabilization and motor control rather than aggressive stretching into end ranges that may feed the hinge pattern.
2) Technique selection for manual care
Some patients report temporary relief from manual therapy, followed by rebound symptoms. Motion data can help determine whether certain levels should be protected and whether gentler techniques are appropriate while stability is rebuilt.
3) Better trigger management
If symptoms flare with rotation + extension (for example, checking blind spots and looking up), the plan may include temporary reduction of those combined arcs, plus ergonomic and driving modifications to reduce cumulative stress.
4) Coordinated referrals
Because pulsatile tinnitus can involve vascular and ENT causes, many cases require collaboration. Motion findings can help clarify when cervical stabilization is a reasonable part of the plan, alongside appropriate ENT/vascular evaluation.
Practical tracking that makes DMX more useful (general guidance)
If you’re considering DMX or preparing for a consult, track these for 7–10 days:
- triggers: rotation left vs right, extension, flexion, combined movements.
- time of day: morning vs afternoon vs night.
- posture load: driving minutes, screen time.
- modulation: does gentle traction help? does pressing the neck change it?
- intensity scale 0–10 and whether you can “turn it down” with a position.
This trigger map helps providers match findings to real life rather than treating the report as an abstract document.
Safety and red flags
Pulsatile tinnitus can be associated with conditions that should be evaluated urgently. Seek urgent evaluation if you have:
- sudden severe headache (“worst of life”).
- neurological changes (weakness, facial droop, speech change).
- vision loss or double vision.
- fainting.
- new severe imbalance.
- new severe neck pain after trauma.
FAQs
Can the neck cause pulsatile tinnitus?
In some cases, symptoms can be influenced by cervical posture and motion, especially when tinnitus changes with head position. However, medical causes must be evaluated as well.
Why would MRI be normal if symptoms are strong?
MRI is a static study. If the symptom is triggered by motion behavior, static imaging may not capture translation/angulation patterns that appear during movement arcs.
What does DMX add?
DMX evaluates real-time motion behavior through guided arcs, allowing assessment of translation, angulation, symmetry, and hinge patterns.
Does DMX replace ENT or vascular evaluation?
No. DMX complements evaluation when motion dependence suggests cervical mechanics may be contributing, but medical evaluation is essential for pulsatile tinnitus.
References
- Cleveland Clinic: Patient education on tinnitus and pulsatile tinnitus.
- PubMed-indexed literature on whiplash-associated disorders, cervical biomechanics, and cervicogenic symptom patterns.
Learn more: Treatment
Schedule your appointment today:Appointments
Call 305-275-7475 orbook your appointment online
Dr. Rodolfo Alfonso, D.C.
Dr. Mark N. Berry, D.C.
Sunset Chiropractic and Wellness
8585 Sunset Dr. STE 102
Miami, Florida 33143