If standing still quickly triggers low back pain but walking feels better, your pattern may be load-sharing and stability related. Standing concentrates pressure and reduces the circulation ‘pump,’ while walking redistributes load. DMX evaluates lumbar motion behavior (translation/angulation, hinge patterns) to help clarify motion-dependent drivers when static imaging doesn’t match function.
- Standing still can be more provocative than walking because it concentrates load and increases pooling.
- This pattern often reflects mechanics and stability demand, not just tight muscles.
- DMX can document motion behavior that supports stabilization-first rehab planning.
Last updated: April 14, 2026
Reviewed by: DMX Miami clinical team
Introduction
One of the most consistent mechanical patterns in low back complaints is: “Walking is okay, but standing still destroys me.” People report pain while cooking, showering, standing in lines, or washing dishes, yet they can walk longer with less pain. We see this across Miami, Fort Lauderdale, Miami‑Dade, Broward, and the Florida Keys, and in visitors from the USA, Colombia, Chile, Argentina, Mexico, and the Caribbean. When symptoms are tied to posture load and stillness, the case is often mechanics-first.
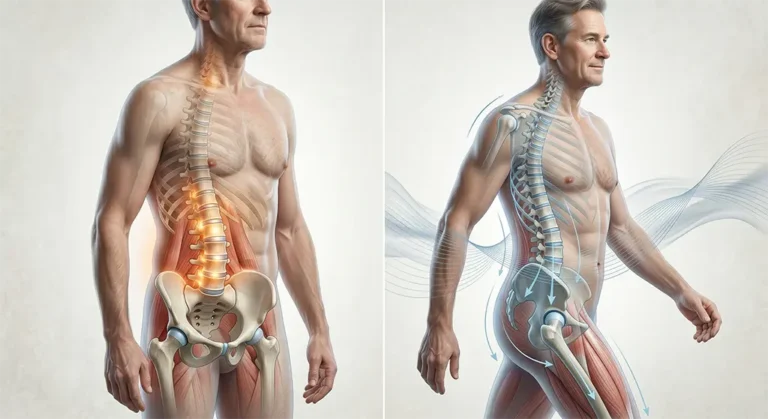
Why standing still is uniquely provocative
Standing still concentrates load into the same tissues. Unlike walking, you don’t redistribute pressure through the hips and legs. You also lose the muscle “pump” that helps circulation and reduces pooling. If a segment is sensitive or unstable, the constant demand can trigger guarding and pain.
The load-sharing concept
Healthy movement shares load across multiple segments. If one segment hinges or moves excessively, it becomes overloaded during standing. That can produce rapid pain build-up, a beltline ache, relief when you sit or lean, and temporary relief with walking.
Why MRI can be unrevealing in standing intolerance

MRI is usually supine, reducing load. Standing intolerance is upright load dependent. A hinge pattern may not be obvious on a still scan, especially if the driver is motion sequencing and instability behavior rather than a single structural lesion.
What DMX evaluates
DMX evaluates real-time lumbar motion behavior through guided arcs and can document translation and angulation patterns, hinge segments, and sequencing issues. This supports a stability-first plan tailored to your trigger pattern.
How DMX findings can guide a better plan
With motion clarity, providers can:
- Prioritize stabilization and endurance
- Modify hinge training and lifting strategy
- Change stretching that may feed extension intolerance
- Set milestones: longer standing tolerance, fewer flare-ups, improved transitions
Practical strategies (general guidance)
- Use micro-movement while standing: ankle pumps, calf raises, weight shifts
- Use short sit breaks before pain peaks
- Break up standing tasks (cook in phases)
- Track whether pain worsens with slight lean-back posture
Safety note
Seek medical evaluation for red flags: progressive weakness, bowel/bladder changes, severe numbness, fever, trauma with severe pain.
FAQs
Why does standing still hurt more than walking?
Standing concentrates load and reduces circulation pumping; walking redistributes load and improves tissue ‘pumping,’ often reducing symptoms.
Does this mean I have instability?
Not always, but standing intolerance can reflect load-sharing and stability demand. Evaluation helps clarify.
What does DMX add?
Real-time lumbar translation/angulation and hinge patterns through guided arcs.
Does DMX replace MRI?
No. It complements MRI/CT/X‑ray when motion and stability are the key questions.
References
- AAOS OrthoInfo: Mechanical low back pain and posture/load education.
- PubMed-indexed literature on lumbar segmental motion and instability concep
Learn more: Treatment
Schedule your appointment today:Appointments
Call 305-275-7475 orbook your appointment online
Dr. Rodolfo Alfonso, D.C.
Dr. Mark N. Berry, D.C.
Sunset Chiropractic and Wellness
8585 Sunset Dr. STE 102
Miami, Florida 33143